How can we tell the difference between men and women? At a basic level we are distinguished by our genitals. This is a simple answer, but not as accurate or useful in social situations. Instead of relying entirely on physical characteristics to identify individuals as male and female, we use other clues. Clothing, secondary sex characteristics and things that emphasize secondary sex characteristics encourage us to accentuate the psychological, emotional, mental, and behavioral differences.
In our examination of gender we will now highlight the psychological aspects of being male and female. However, we will observe how slight abnormalities or changes at the biological level can influence the psychological and social levels of analysis. In this lecture we will examine the topics of studying gender and gender roles, gender role learning, contemporary gender roles, and gender variation.
There are several key terms for this chapter. Sex is whether one is biologically female, male, or intersex. Genetic sex is the chromosomal and hormonal sex characteristics. For example, whether one's chromosomes are XY or XX or something else and whether estrogen or testosterone dominates the hormonal system. Anatomical sex is the physical sex including gonads, uterus, vulva, vagina, or penis. Although "sex" and "gender" are often used interchangeably, gender is not the same as biological sex. Whereas sex is rooted in biology or anatomy, gender is rooted in culture. Gender, or femininity or masculinity, relates to the social and cultural characteristics associated with being male or female. Sub terms of gender include assigned gender, gender identity, and gender role. Assigned gender is given by looking at your genetalia and is based on whether you have a penis or vagina. It influences how others resond to you but determining that you should be treated as either a male or female. Gender identity is a person's internal sense of being male or female. For most, gender identity is permanent and congruent with sexual anatomy and assigned gender. Gender roles are the attitudes, behaviors, rights, and responsibilities that society associated with each sex. Gender role is influenced by culture, age, ethnicity, and environmental factors that determine gender-related patterns of behavior.
Biological males are expected to act out masculine gender roles, and biological females are expected to act out feminine gender roles. Gender role stereotype is the rigidly held oversimplified beliefs about how each gender should behave. Gender role stereotypes tend to be false or misleading for individuals of the group and the group as a whole. They are statistically valid generalizations that do not predict facts.
Gender role attitude is the belief one has for self and others on what's appropriate for male or female traits and activities. Gender role behavior is the actual activities or behaviors a person engages in as a female or male. And gender presentation is what is perceived by others through one's bodily habits or personality.
Gender is developed through the interaction of its biological and psychosocial components. The genetic and anatomical sex is the biological aspect, and the assigned gender and gender identity are the psychosocial aspects. Because these dimensions are learned together they seem to be natural.
For example, if a person looks like a girl, biologically, believes she should be feminine, culturally, feels as if she is a girl, psychologically, and acts like a girl, socially, then her gender identity and role are congruent with her anatomical sex.
But what if these dimensions were incongruent? This results in gender variations. Gender variations are deviations from the two normal genders emphasized by most cultures. Individuals who are gender variant cannot or choose not to conform to societal gender norms associated with their biological sex. They are also known as gender identity disorder or gender dysphoria. However, what makes a person a man or woman goes beyond simple anatomy.
Biology creates males and females, but it is culture that creates our concepts of masculinity and femininity and its inherent fluidity and complexity.
In Western society, we see the sexes as polar opposites. This view is reflected in the popular terminology opposite sex. We associate different qualities with different genders. Our traditional gender stereotypes fit this pattern of polar opposites.
Men are characterized as being aggressive, rational, embody instrumentality, task-oriented, and want sex. On the other hand, women are characterized as passive, irrational, embodying expressiveness, emotion-oriented, and want love. Stereotypes reflect the probabilities that a woman or man will have certain characteristics based on gender.
Gender stereotypes developed during childhood can be carried into adult lives and possibly result in sexism. Sexism is the discrimination based on sex rather than individual merits. Sexism is often associated with gender stereotypes and may discourage individuals from expressing their full range of emotions or seeking certain vocations. These identities are combination of nature and nurture. Some qualities are biologically based and some are culturally based.
Let's examine the definition of sexual orientation. It is the pattern of sexual and emotional attraction based on the gender of one's preferred partners.
Now let's address gender and sexual orientation. Gender, gender identity, and gender role are conceptually independent of sexual orientation. However, many assume they are closely related. Heterosexuality has been assumed to be a critical part of masculinity and femininity. Masculine men are attracted to women and feminine women are attracted to men. Along with this perception, two beliefs about homosexuality exist. Some believe that gay men can't be masculine and lesbian women can't be feminine. These beliefs imply that homosexuality is associated with a failure to fill traditional gender roles.
These negative stereotypes, which hold that people fall into distinct genders, with natural roles, and are presumed to be heterosexual, are referred to as heteronormativity, and merely fuel homophobia.
It is difficult to analyze the relationship between biology and personality because learning begins at birth. During infancy and early childhood, children's most important source of learning is the primary caregiver. Many parents are not aware that their words and actions contribute to their children's gender-role socialization. Nor are they aware that they treat their daughters and sons differently because of their gender.
Children are socialized in gender roles through several very subtle processes:
Manipulation is when parents treat boys and girls differently. They treat a daughter gently and tell her she is pretty. They treat a son roughly and advise him that big boys do not cry. Channeling is when children's attention is directed to specific objects. Toys, for example, are differentiated by sex. Dolls are considered appropriate for girls, and cars for boys.
Verbal appellation is when parents use different words with boys and girls to describe the same behavior. A boy who pushes others may be described as "active," whereas a girl who does the same is usually called "aggressive."
Activity exposure is the type of activities boys and girls are encouraged to be exposed to and imitate. For example, boys are discouraged from imitating their mothers, whereas girls are encouraged to be "mother's little helper."
Image from McGraw Hill Image Library

Teachers serve as socializing agents in daycare centers, nursery schools, and kindergartens. Females are often more common in these venue and may reinforce ideas that women are concerned with children and men are not. They encourage different activities and abilities in boys and girls. For example, contact with sports, math, and science are for boys and gymnastics and language skills are for girls. Peers define gender role norms through play activities and toys. Girls play with dolls, babies, or want to be glamorous women. Boys play with video games in which they kill and maim to dominate and win. Peers influence the adoption of gender role norms through verbal approval or disapproval. The perceptions of friends' attitudes, behavior, and beliefs encourage them to adopt similar ones to be accepted. And last but not least, the media as a socializing agent promotes and condones negative stereotypes about gender, ethnicity, age, and ability, as well as sexual orientation. To the right you can see an ad that was run in J.Crew in 2011. In the ad, the president of J. Crew is painting her son's toes with neon pink nail polish. This ad sparked a lot of controversy and was discussed on all major news stations. Debate was regarding the gender-appropriateness of the mother painting her son's toes pink. The controversery highlights the media's role in defining gender-role appropriateness and people's comfort when these traditional roles are defied or challenged. Image: http://www.alllacqueredup.com/2011/04/controversial-jcrew-pink-nail-polish-ad.html#.Ubcwuvmcdx4
Culture exaggerates or creates differences between females and males when they may be minimal or nonexistent. This is done by creating a schema. Gender schemas are interrelated ideas which help information processing by categorizing in a variety of ways.
Schemas emphasize the male and female dichotomy, undermining and undervaluing the uniqueness of the individual. They are used in many life dimensions, for example, activities, emotions, behavior, clothing, and even colors. Being nurturing, having compassion, playing with dolls, wearing dresses, and even colors of pink are associated with women. On the other hand, fighting, having anger, playing with action figures, wearing pants, and the color of blue is associate with being male.
Gender schemas are important in cultures. They make multiple associations between gender and other non-sex-linked qualities, like affection and strength. They make gender distinctions important, and they are used as a basis for norms, status, taboos, and privileges. Men have leadership positions and are sexually assertive, and women are homemakers and are sexually passive. These are the schemas associated with genders in our culture.
Traditional gender roles have changed. Today an egalitarian approach to gender roles exist and includes diverse groups. Women's roles have changed more than men's. Changes affect all socioeconomic classes. For men, traditional male roles are instrumental or involve practical or task-oriented traits. They are expected to conform to the stereotypical expectations of success, competition.
Sexual scripts are acts, rules, and expectations associated with how we are to behave sexually when acting out our gender roles. Male sexual scripts often include common myths in terms of the separation of sex from love and attachment. Sex is seen as a performance. The traditional male sexual script includes these characteristics: men should not have or express certain feelings, performance is the only thing that counts, the man is usually in charge and always wants sex and is ready for it, all physical contact leads to sex for men, and sex equals intercourse and sexual intercourse leads to orgasm.
The traditional female gender role highlights characteristics such as passivity, physical attractiveness, and being a wife and a mother. However, there are striking ethnic and individual differences. American middle-class white women could serve as wives and mothers but were not expected to defer marriage for career goals. Their gender role now includes work outside the home, but subordinated to marital and family roles. African American gender roles are more egalitarian for men and women. Latina women must be faithful and subordinate to their husbands while maintaining family traditions and culture. Asian Americans' gender roles include conservative attitudes about sexual behavior and norms, but these are changing with the increased exposure to American culture. Female sexual scripts focus on feelings over sex and on love over passion. For example, sex is good as well as bad, and it is not okay to touch yourself down there. Sex is seen for men and men should know what women want. Women shouldn't talk about sex and should look like models and are nurturers. They give, and men receive, and there is only one right way to have an orgasm___vaginal sex.
In recent decades, there has been a significant shift toward more flexibility in gender roles. Traditional hierarchical gender roles is when one sex is subordinate to the other. Egalitarian roles are when both sexes are treated equally. Androgynous roles are when both sexes display the instrumental and expressive traits previously associated with one sex .
Although women's roles have changed more than men's, men's are also changing, and these changes seem to affect all socioeconomic classes. Contemporary gender roles are evolving from traditional hierarchical gender roles to egalitarian and androgynous roles, displaying a combination of traits from each type. These changes are influenced by individual differences, situations,and stages in life.
All images from McGraw Image Library
There are more balanced sexual attitudes and behaviors for males and females in contemporary sexual scripts. More recognition is given to female sexuality. The sexual scripts are relationship-centered rather than male-centered. Some characteristics include sexual expression is positive; sexual activities involve a mutual exchange of erotic pleasure; sexuality is equally involving and both partners are equally responsible.
Legitimate sexual activities are not limited to intercourse but include a wide variety of sexual expression, and sexual activities may be initiated by either partner. And both partners have a right to experience orgasm, whether through intercourse, oral-genital sex, or manual stimulation. Additionally, non-marital sex is now more acceptable within a relationship context, yet women are still not granted full sexual equality with males regarding non-marital sex outside the context of a relationship.
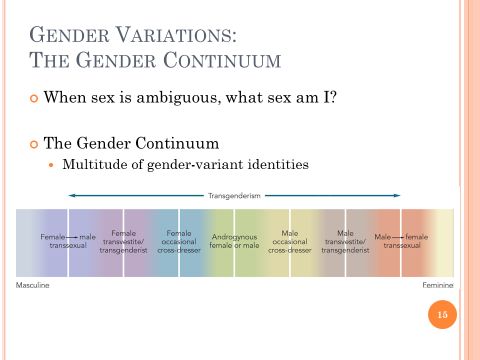
Most of us question our femininity and masculinity but not whether we are male or female. However, for gender variant individuals, "what sex am I?" is a real and painful question. For the topic of gender variations we will discuss transgenderism, disorders of sexual development and intersex, the unclassified form of abnormal development, gender identity disorder, and transsexuality. The answer to the question "what sex am I?" reinforces that psychosexual development is influenced by a multiple factors including exposure to androgens, sex chromosome genes, brain structure, as well as social circumstance and family dynamics.
The Gender Continuum is a contrast to the binary gender view. The concept of gender is on a continuum with a multitude of gender variant identities.
Image from McGraw Hill Image Library
Transgenderism is an inclusive category. Some cultures recognize that sex and gender are not always divided along binary lines, such as male and female or homosexual and heterosexual. Transgender is currently the umbrella term for those who do not conform to traditional notions of gender expression. In North America, a paradigm shift has occurred that challenges the male/female dichotomy of gender. The transgender phenomon embraces the possibility of numerous genders and multiple social identities. This paradigm shift regarding gender has implications for the clinical management of gender identity disorder. Treatment is open to the possibility of affirming a unique transgender identity and role.
The term intersex means various conditions in which a person is born with reproductive or sexual anatomy that does not fit the typical definitions of female or male. Disorders of sex development are congenital conditions in which the development of chromosomal, gonadal, or anatomical sex is atypical. Other labels include pseudohermaphroditism, hermaphroditism, sex reversal, and gender-based diagnostic labels.
The cause of these anomalies is the disruption of the genetic or hormonal process that causes fetal tissues to become male or female and usually occurs in week seven or eight of development. This causes ambiguous genitals to develop. An individual can be born with sex chromosomes, external genitalia, or an internal reproductive system that is not considered standard for males or females.
Even if sexual determination occurs normally, abnormal sexual differentiation can occur. It can occur as an underdeveloped penis or enlarged clitoris (CLIT-oris), or even a small penis. Individuals with these anomalies are shrouded in secrecy by families and medical establishments in the past, but now things are slowly starting to change.
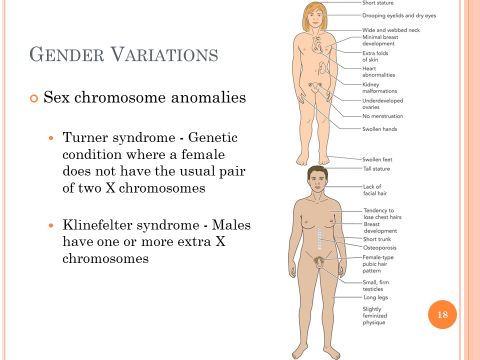
Two syndromes resulting from erroneous chromosomal patterns may result in gender confusion. We will discuss:
Turner syndrome
Klinefelter syndrome In both of these, the body develops with some marked physical characteristics of the other sex.
Turner syndrome is described as females who lack a chromosome and are described as XO rather than XX or XY. The individual has a female external appearance but no ovaries. Therfore, changes initiated by ovarian hormones cannot take place. The body does not gain a mature look or height and menstruation cannot occur. These individuals may have academic problems and poor memory and attention. Treatments include hormonal therapy and assisted fertility. The hormonal therapy includes androgen, estrogen, and human growth hormone therapy, replacing the hormones to produce adolescent changes. Unfortunately, the female will likely remain infertile.
Klinefelter syndrome is related to males. These individuals are males who have an extra X chromosome. For example, the could be XXY or XXXY or XXXXXY rather than XY. The testes of these males are small and firm, and they also have some female physical traits. Many men with Klinefelter syndrome are never diagnosed. The physical traits include tallness, breast development, sparse body hair, and/or a small penis and testes. They tend to exhibit learning disabilities and also have lower testosterone levels which cause low sex drive, the inability to experience erections, and infertility. Treatment includes testosterone replacement. This prevents osteoporosis, maintains physical energy, sexual functioning, and well-being, and in-vitro techniques can allow some to become a biological father.
Images from McGraw Hill Image Library
Hormonal imbalances may cause males or females to develop physical characteristics associated with the opposite sex. When a person who is genetically male is resistant to male hormones or androgens, he is said to have androgen insensitivity syndrome. The male has female genitals but no female internal organs. At puberty the male develops hips and breasts and other secondary sex characteristics, but no public hair and no menstruation. <br /><br />The testes also remain in the abdomen and are sterile. He is assigned a female gender status at birth and many experience female gender identity. They develop as a female; then the physical anomaly is discovered at puberty. Treatments include removal of the undescended testes and estrogen replacement therapy. <br /><br />Another hormonal disorder is congenital adrenal hyperplasia. This is when a genetic female with ovaries and a vagina who develops externally as a male. This is due to the malfunctioning of the adrenal gland, which produces androgen instead of androgen-inhibiting cortisone.
At birth the child has ambiguous genitalia, a penis with an empty scrotum or an enlarged clitoris with or without a vaginal opening. In the past doctors and families choose to assign female gender at birth and treatment is given to promote female development. However, the gender role behavior is masculine, and there is a higher likelihood of the female experiencing homoerotic dreams and sexual attraction.
Of unknown origin, but in some cases passed down through families, is a condition called hypospadias. This is when the opening of the penis is located somewhere on the underside of the glans, the shaft or at the junction of the scrotum. Infants with hypospadias should not be circumcised. Surgery, which consists of straightening the penis and correcting the hypospadias, is usually done before the child is 18 months old.
According to the American Psychiatric Association, gender identity disorder (GID) consists of a strong and persistent cross-gender identification and persistent discomfort about one's assigned sex. This diagnosis is not made if the individual has a concurrent physical disorder of sexual development or intersex condition. Furthermore, there must be clinically significant distress or impairment in social, occupational, or other important areas of functioning.
The first step is usually psychotherapy, although psychotherapy is not always required for medical treatments. Traditional medical treatment for gender identity disorder has included three phases:
a real-life experience in the desired role
hormones of the desired gender
surgery to change the genitalia and other sex characteristics
Image from McGraw Hill Image Library
Gender identity disorder can be difficult to identify and come to terms with for individuals and their families. This is a short YouTube clip from a TLC's Strange Sex. To view the video please click on the image.
In this video, I want to you ask yourself these questions: What sort of childhood did Nat have? When did Nat begin to feel incongruent with his assigned sex? How do you think Nat's experience would be influenced if his family support was different?
Image is hyperlinked to a YouTube video: http://www.youtube.com/watch?v=xiHlQ65XPvo
Transsexuality is when gender identity and sexual anatomy are not congruent. It may occur with heterosexual, homosexual, and bisexual orientations. Some cultures accept incongruence and create an alternative third sex. Transsexuals believe they have been given the body of the wrong sex and want to change sex, not their personality. This revolves around issues of gender identity and distinctly is different from homosexuality. Following surgery transsexuals may or may not change their sexual orientation, whether it is toward members of the same, the other, or both sexes. Sexual reassignment surgery is an alternative for transsexuals. It is sought to bring genitals in line with their gender identity and to diminish serious suffering they experience. Male to female operations outnumber female to male operations by five to one ratio. Images from McGraw Hill Image Library
Ordinarily we take for granted that gender is only male or female. However, gender is a complex process involving both biological and psychological elements. We have examined the connection or disconnection between our genitals, our identity, and our feelings of being female or male, as well as its relationship to sexual orientation and how gender is learned. We have found few significant inherent differences exist between the sexes. Because people sometimes react negatively to variations simply because they are fearful or ignorant, educating others about disorders of gender, orientation, and sexual differences may help to reduce their fear and ignorance and the stigmatization that accompanies both.