So in this lesson we're going to talk about the prevalence of obesity, or how common obesity is, as well as defining the terms overweight and obesity. We'll talk about the health risk of being either overweight or obese. We'll talk about ways that we measure body composition, or how our body is-the tissues our body's composed of. We'll identify factors that contribute to obesity, and finally, we'll talk about some skills for maintaining a healthy weight.

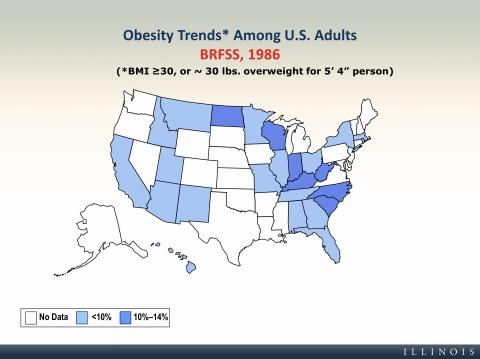
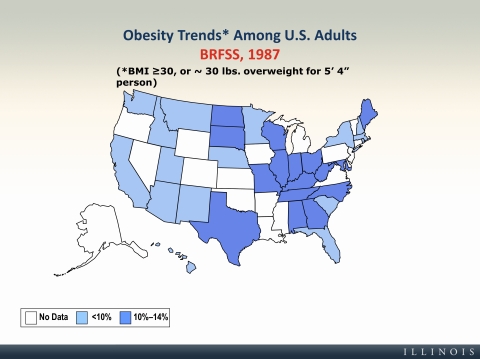
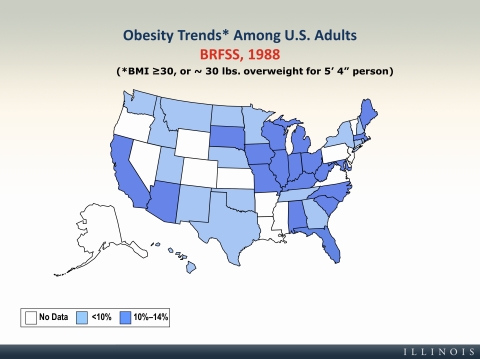
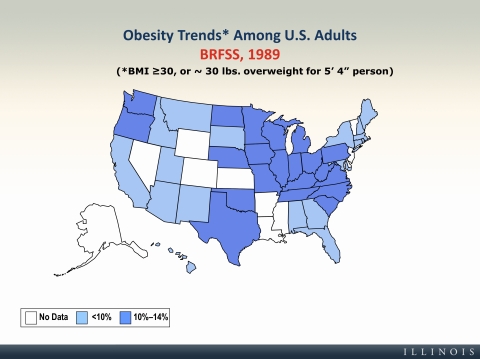
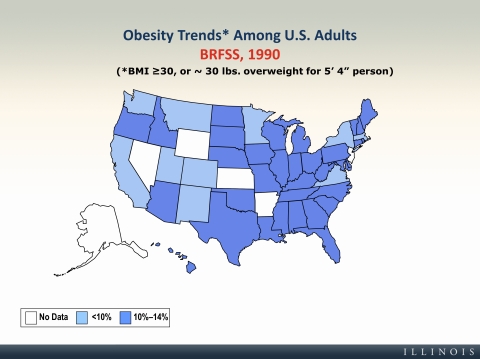
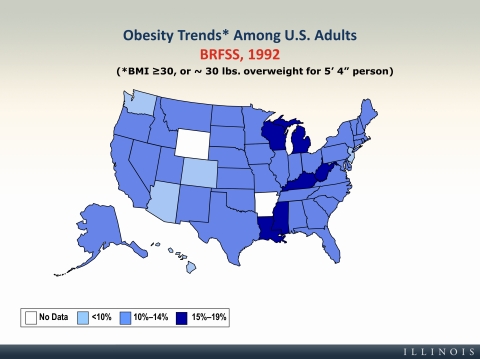
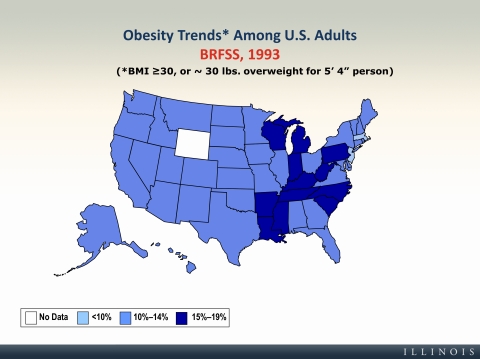
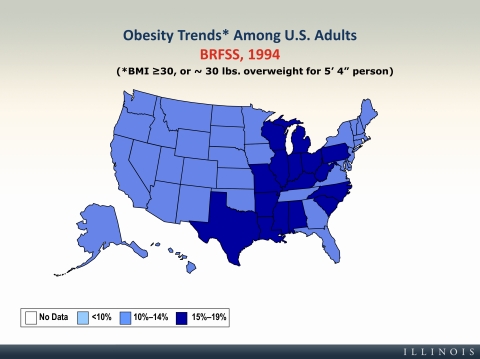
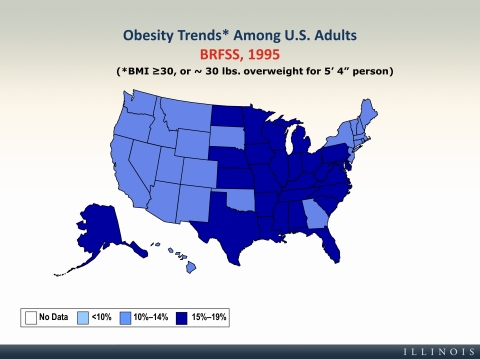
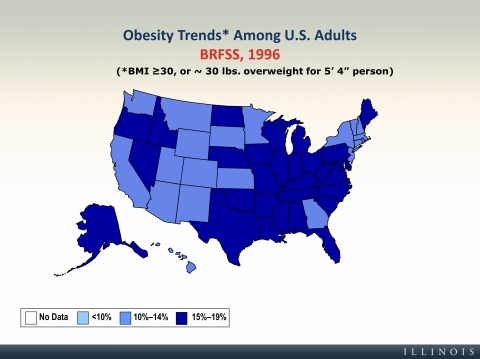
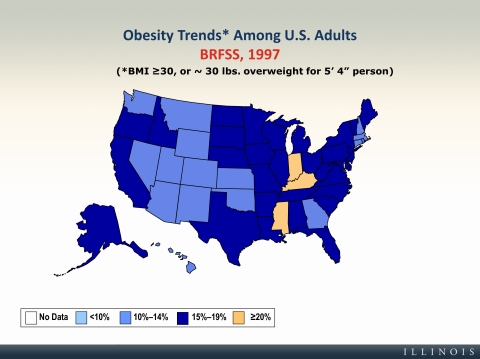
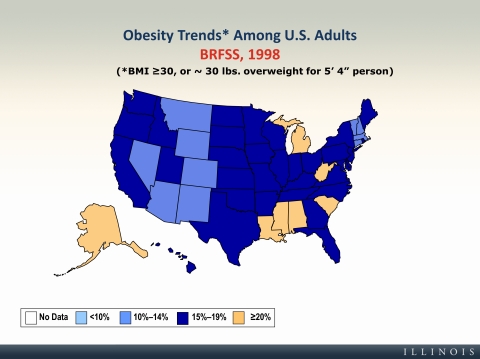
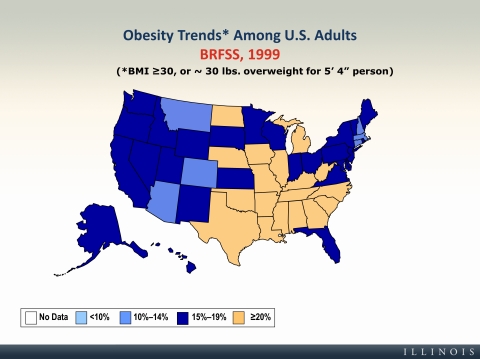
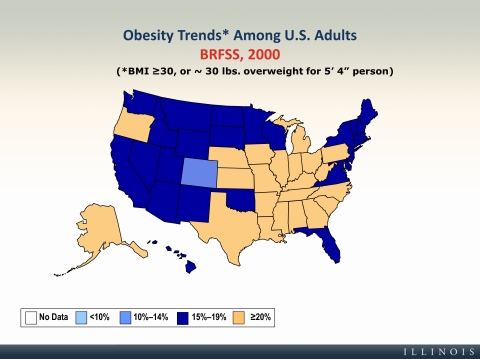
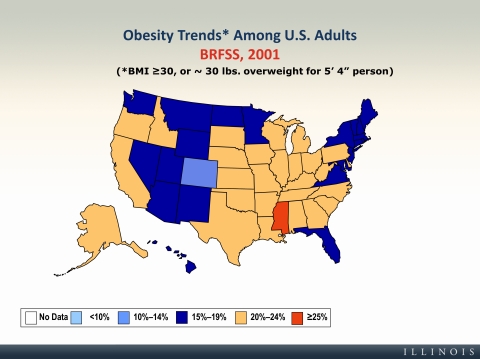
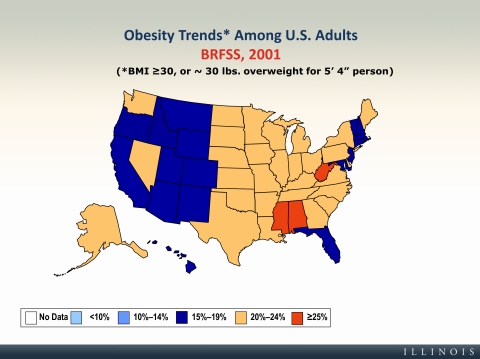
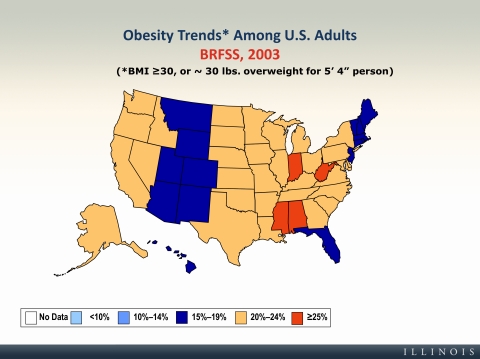
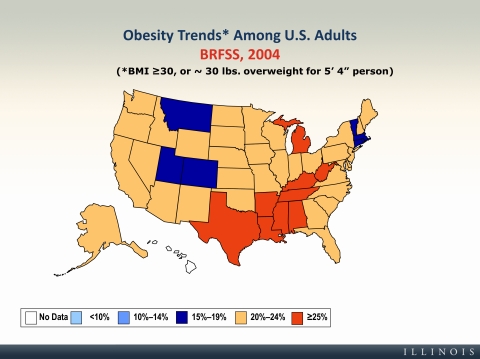
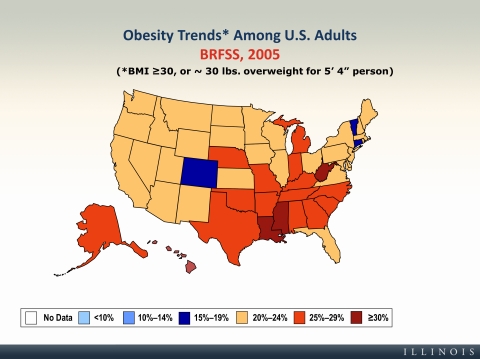
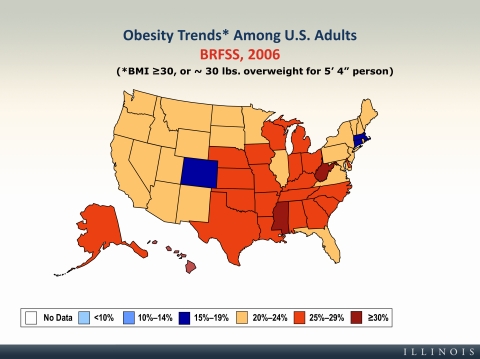
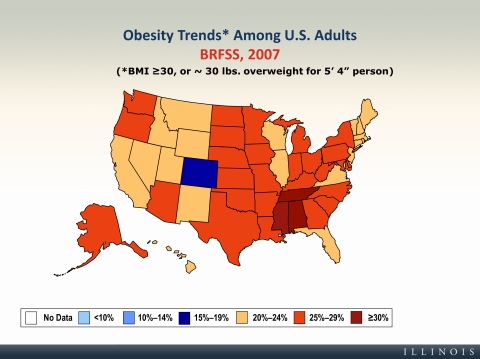
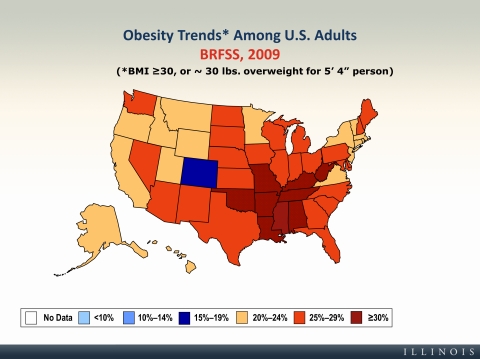
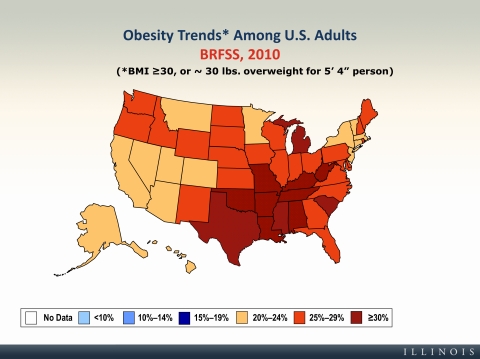
We'll start this lesson with a visual display of the trends in obesity, ranging from 1985 through 2010. And on this slide you can see comparisons of obesity trends, we're talking about people with a body mass index of greater than or equal to 30, or about 30 pounds overweight for a 5'4" person, as you see here on this slide.
And so here you can see maps for 1990, 2000, and 2010, but the next several slides in this PowerPoint show you the progression year by year and state by state in the increases in obesity. So I want you to take a few moments and flip quickly through these maps on the next several slides and watch our nation becoming more and more obese over this relatively short period of time. Take a few minutes, flip quickly through this, and watch as the colors change progressively from white, light blue, to yellow, and then finally to red, where we are today in most states. Just watch that progression of becoming more and more obese.



So what did you see when you looked at all those maps? Clearly our country's becoming more and more obese, but what else did you see? What did you notice?
I'll cover a few points here that you should note. The first is that remember that these graphs are only indicating the changes in obesity, not in people who are overweight, and we'll define the difference between those two, but essentially obesity is a greater level of being overweight. So it's just a higher degree of being overweight, and so this map does not even capture the people in our country who are simply overweight.
You probably also noticed regional differences. So, the South and the Southeast, in particular, seems to change before the other areas of the country. And I want you to think about what some possible reasons or influences on these changes might be. It certainly could have to do with the type of food that is typically eaten in these situations or these locations in the country, maybe the cultural beliefs or practices, but what else can you think of?
Another point to note is that we have an obesity epidemic in this country. Obesity rates have changed very quickly. You looked at time-at how much they've changed since 1985, which seems like a long time ago, but really in the grand picture it's not that long ago. And so we've seen these rapid increases in obesity. And if you click on the obesity epidemic bullet point here, I want you to watch a video that was produced by the CDC. It talks about this epidemic. And in the video they talk about childhood obesity as well, and so the maps that you saw were only for adults in the United States, not for children. But, unfortunately, we're seeing these same problems in children.
As you saw in the video, if you just watched it, about one in six children are now obese, and about one in three young people, which is ages 6 to 19, are at risk of becoming overweight or obese. And because of this we're seeing health problems, like type 2 diabetes, in children that we only used to see in adults. So clearly we have a problem with obesity and overweight trends in this country, and we'll cover some more of these topics as we go through the slides here today.
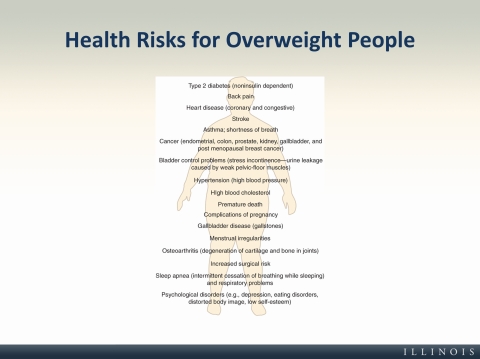
So why do we care is people are overweight or obese? Well, you can see here this laundry list of diseases that you are at higher risk for if you are overweight or obese. They include type 2 diabetes, back pain, heart disease, cancer, osteoarthritis, problems sleeping, psychological disorders. So these health risks range a wide variety of influences, and they affect different parts of your body, and so really treating obesity related diseases is not only bad for the individual, but it also costs us billions of dollars (and that's billions with a "b") every year. About ten percent of all healthcare costs are due to treating these health risks for overweight or obese people. So clearly the epidemic has both an individual cost and a societal cost.
So let's take a step back here and let's define what I mean by overweight and obesity. These are both classifications that represent a weight that exceeds the threshold of a health criterion in a relationship to morbidity and mortality. In other words, these are weights that are associated with increased risk of disease or death.
And overweight is a body weight that's greater than or equal to ten percent over the ideal weight for a specific height. So, for someone that's a particular height, we can predict their ideal weight. Anything that's ten percent over that would be considered "overweight."
Obesity, again, is based on an ideal weight for a specified height, but we're talking about someone who is greater than or equal to 30 percent over that ideal weight.
It's important to note here that these are not measures of body composition or whether your body is made up of fat or lean tissue, but just a ratio of weight to height, and they don't take into account the type of tissue, only your overall weight.
One very common indicator of overweight or obesity and also of health risk is body mass index, or BMI. And that's simply defined as your body weight in kilograms divided by your height in meters squared. And this is an indication, again, of the ratio of your weight to your height, and it correlates very well with the amount of body fat, but it is not a measure of body fat. It's simple, quick, inexpensive, so it can be used in many different clinical and practical settings. But again, it's important to understand that it's not a measure of body fat, only a measure of your ratio of weight to height. So can you think of any problems with using solely a BMI to determine whether someone's at health risk because of their weight? Again, it's only an estimate of body fat, and it also doesn't provide any information about how the fat is distributed in the body, which is also an important to know for health risk. Alternatively, someone that is very muscular could have a high body mass index but not be at health risk. But the reality is is that the little error that there is there in maybe classifying someone who has lots of muscle with a higher body mass index is not nearly as big of a problem as our obesity problem. So BMI is a pretty good, quick, easy, simple measure of health risk and an indicator of overweight or obesity.
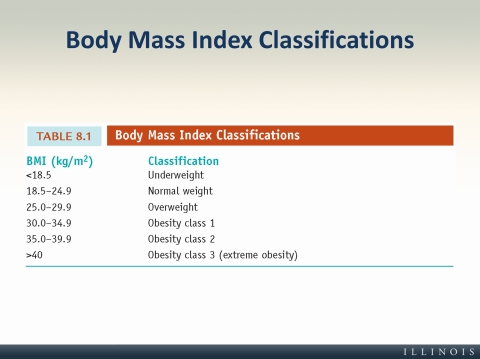
Here you can see the body mass index (or BMI) classifications, ranging from underweight through obesity class 3 (or extreme obesity), and what you see here is that as your BMI increases, your level of risk increases as well. And that's risk of diseases and mortality, or death. And this general BMI chart can be used for both men and women, aged 20 years and older, so adults, both men and women. And we use special charts for anyone that's under 20 because you take into account the sex of the person and the growth patterns as well. But in general this is the table that we'd use for adults.
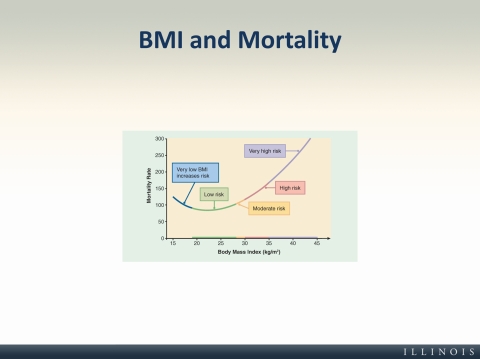
This graph shows the mortality rate in relation to body mass index, and here again, mortality rate, we're talking about a risk of death. You don't have to worry about the particular numbers here, but again, you can see that at the very low BMI you have an increased risk of mortality. The lowest risk is in kind of a normal body mass index range, and then it just gets higher and higher as your body mass index increases. And so it's important to note here that the biggest risks come from increases in body mass index.
And this very low end of the BMI, it does increase your risk, but that probably takes into account people who are quite unhealthy to begin with, and not necessarily just because of their weight. So, for example, maybe an elderly person who's also suffering from some kind of chronic disease but has a very low weight, or, for example, someone who has an eating disorder, very low weight. So that low BMI is an increased risk, but oftentimes it's confounded with people who have other diseases. And the biggest thing to note here is that, in general, as BMI increases, your risk of death also increases.
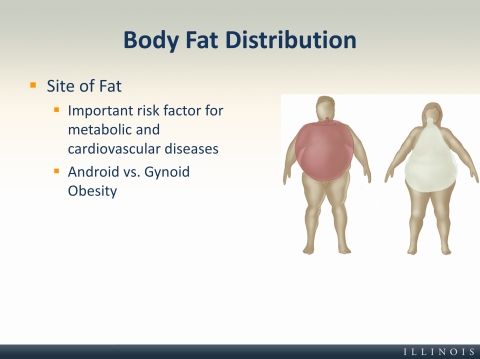
As I mentioned briefly before, the location of the fat in your body, or the body fat distribution, is also important to note. And so we have two different body types, and you can see them on the slide here. On the left you have your android (or apple shaped) where the fat is more centrally located, and on the right you have gynoid obesity (or the pear shape) where the fat is mostly around the hips and the butt and below the waist. The apple shape is associated with a higher risk of disease because that fat is surrounding all of the internal organs. And we know that where your fat is distributed may be even more important than how much fat you actually have.
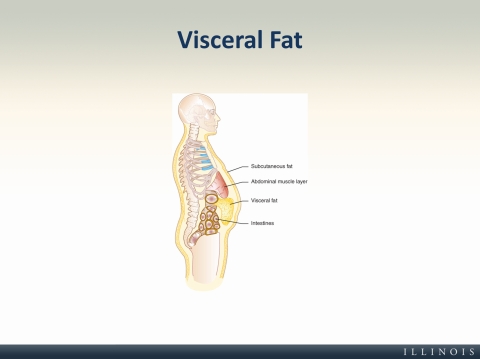
So the type of fat that surrounds your internal organs that we were just talking about is called visceral fat. And you can see it pictured here. It's nestled in all around your internal organs, and that visceral fat is really the dangerous kind of fat. And we don't want to think of fat as a tissue that's just a big blob and does nothing. The problem with fat is that it's a metabolically active tissue. So it's producing chemicals and hormones that may interfere with your normal bodily processes. So we know that this visceral fat is really the dangerous kind, and that's why being an apple shape as opposed to a pear (or an android opposed to a gynoid obesity) is more dangerous or puts you at higher risk for diseases.
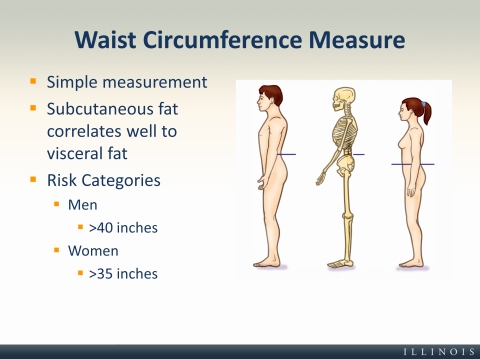
So another way to access risk is by measuring someone's waist circumference. And here we're trying to get at where your fat is distributed. This again, just like BMI, is a very simple measurement, and it really measures subcutaneous fat, or fat that's right under the surface of the skin. But this subcutaneous fat correlates very well to the amount of visceral fat that you have. So although we're not directly measuring visceral fat here, the kind that's inside around your organs, it is a pretty good-it is associated with how much visceral fat you have when you do this waist circumference measure.
And you can see here in the picture where we would take this measure on a female and a male. And really all you need to do this is a tape measure. Simple and easy. And you can see the risk categories on the slide here. For men having a waist that is greater than 40 inches and for women having a waistline that's greater than 35 inches indicated higher risk of diabetes, hypertension (which is high blood pressure), cardiovascular disease, and other weight-related diseases.
The previous two measurements that we talked about -BMI and waist circumference—are really good, easy, quick measures of health risk. But sometimes we want to know a little bit more about the tissues that make up your body. And so that's what we define as body composition. It's allowing you, when you measure body composition, it's allowing the researcher or the clinician to assess the percentage of fat versus the percentage of fat free tissue that someone has in their body.
And so fat is the first type of tissue. We have both essential and storage fats. The essential are the amount of fat that your body absolutely needs to do all of its proper functioning, and then storage fat is anything that you are essentially stockpiling on top of those essential fats.
The other type of tissues you would have in your body would be fat free tissue, and so when you do a body composition measurement usually you get a percentage fat and a percentage fat free tissue. The fat free includes many different things—muscles, bones, organ tissues, blood, and pretty much everything else except for the fat.

Here you can see the typical differences between a man and a woman in body fatness in both the storage fat and essential fat. And the take home point from this illustration is really that women have both more overall fat, body fat in general. Again, it's possible for a woman to have less body fat than a man, but in general women have higher levels of body fat. They also have higher levels of essential fats compared to men. And this is really due to childbearing and very useful for childbearing purposes.
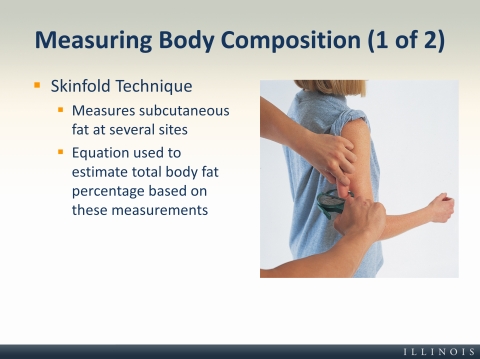
The first measurement that we'll talk about for how we measure body composition is again a very simple technique called the skinfold technique. And here we measure subcutaneous fat at several sites. In the picture you can see the clinician or researcher pinching the skin and fat that sit right under the surface on the back of this young girl's arm with a pair of calipers, and that's essentially what this test does. You measure that with the calipers, you do it at several sites, oftentimes they're different for men and women, and then you use an equation to estimate total body fat based on the subcutaneous fat located in each of these sites. It's easy to perform, but it does require an experienced tester to do this method reliably.
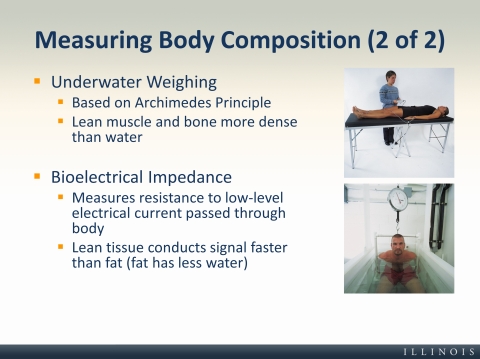
Two other ways that we measure body composition are underwater weighing and bioelectrical impedance. Underwater weighing, which we also know as hydrostatic weighing, is based on Archimedes principle, and that is when a body is submerged in water, there's a buoyant counterforce equal to the weight of the water that's displaced. So, someone with lean muscle and bone, with a lot of lean muscle and bone, will be denser because those tissues are denser than water. So a person with lots of those types of tissues will weigh more in the water than someone who has the same weight on land but a higher percentage of fat in their body. And you can also think of this as fat floats, muscle and bone are denser than water, so a person with lots of those tissues is going to weigh more in the water. The person who weighs more in the water has a lower body fat percentage. So that's the first type.
The second type of way that we measure body composition is bioelectrical impedance, and here we're using a low level electrical current that's sent through the body, and then the resistance to that current by the tissues is then measured. And since lean tissue has more water than fat, it conducts the signal faster than fat. And this test is quick and painless to the participant. The electrical current is not strong enough to cause any problems. So it's quick and painless. The error rate is about three percent. So if someone's body fat composition is measured at 20 percent, their actual body composition is likely to fall somewhere between 17 and 23. And this error is a little bit higher than the 1.5 percent error rate of underwater weighing.
It's also important to note that these are not the only three ways, including skinfold testing, underwater weighing, and bioelectrical impedance. These are not the only ways to measure body composition. We can also do it through x-ray (such as the DEXA machine); air density (oftentimes the Bod Pod it's called) is used. So there are many other ways of measuring body composition, but these are just three that we'll highlight here.
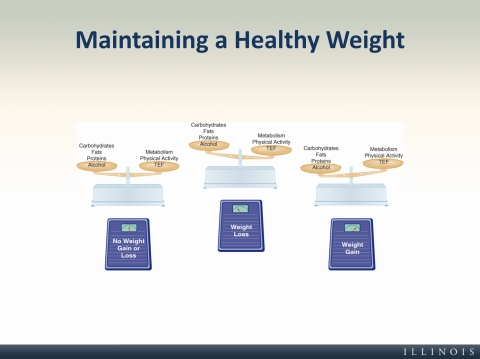
So in the final few slides we'll talk about maintaining a healthy weight. Weight maintenance occurs when there's a balance between your energy intake or the calories that you take in from your essential nutrients, carbs, proteins, fat, and also the nonessential one—alcohol—as well. Alcohol is not an essential nutrient, but it does have calories, so it has to be included in the energy intake category. And you can see on the left here, if you picture this as a scale, you have your carbohydrates, your fats, your proteins, and your alcohol on the left side, and then you also have the energy that you expend on the right side. So when there's a balance between those two things you have no weight gain or loss. You're just maintaining your weight.
And you can see that in the middle when you have weight loss you would be in a negative energy balance, meaning you took in less calories than you expended.
And then finally, on the right you have a weight gain situation, or a positive energy balance, where you're taking in more calories than you are expending. And this is really (on the far right) the problem that most people have in our country, hence the obesity epidemic. Many physiological and psychological factors affect both sides of these scales.
And I want you to take some time to read in your textbook about the role that hunger and appetite play in your energy intake.
And on the next slide we'll talk about the energy that you expend. We'll talk about the right side of these scales.
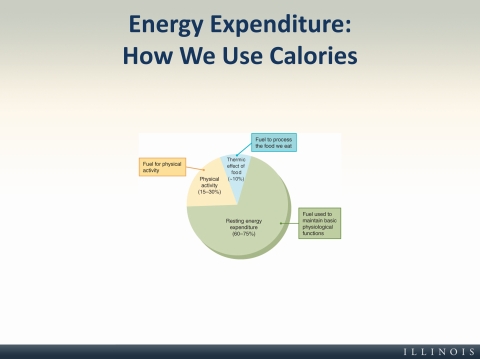
There are three main ways that we expend energy, or you could also classify this as our human metabolism, how we burn energy in our body, or how we use calories.
And the first of these, which makes up about 60 to 75 percent of the energy that we expend, is resting energy expenditure, or your resting metabolic rate. And here this is the caloric requirement to run all of your essential bodily functions while you're at rest. And so this is pretty stable within individuals but differs based on age. So as we get older our metabolism (or our resting expenditure) decreases (gets slower). So we're burning less calories as we get older at rest. It also differs by biological sex. Men typically have higher metabolism than women or burn more calories than women. Thyroid hormones can also-are also strong regulators of this resting energy expenditure. The amount of lean muscle mass we have. So if you have higher muscle mass, you have a higher metabolic rate, you're burning more calories even when you're at rest and not using those lean muscles.
And finally, another factor that can affect (not the only other factor, but one other factor that can affect your resting energy expenditure is if you're in severe caloric restriction. So if you have some reason that you're in a severe caloric restriction situation, your resting metabolic rate is going to go down, so your body's going to try and conserve the energy that you already have in your body when you're essentially starving yourself. So that's the resting energy expenditure, and there are some other differences between individuals, but you can read about those in your book.
The second way that we expend energy is through the thermic effect of food, or the energy needed to eat and process food. And as you can see in the pie chart here, that's only about ten percent, so this is not a way that we really use to increase our energy expenditure. We use that amount to both eat and process the food. It differs based on the type of food you eat. Eating more calories will increase the thermic effect of food, but this is not a great way to increase your overall energy expenditure because you're also increasing caloric intake. And so this is not a category that we talk a whole lot about because it's not very effective for increasing your overall energy expenditure.
And the final category, which we have the most influence on, would be your physical activity. And here it can range anywhere from 15 to 30 percent of your total energy expenditure. And this really captures the energy required to contract and relax your skeletal muscles, and this is the area that differs the most between individuals, and it's the best way to increase your energy expenditure or metabolism. Your metabolic rate increases while you're being active, but the awesome thing is that is also remains elevated after you're done being active. So it's not just during your bouts of physical activity where this-your body's using extra fuel, it also continues after you finish that activity.
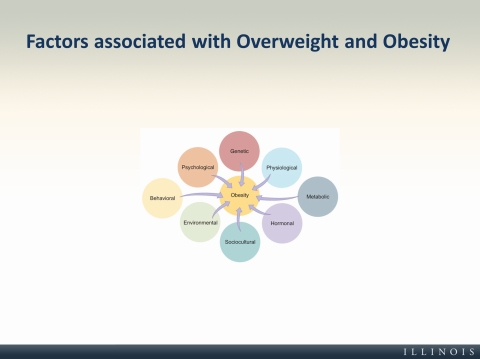
Maintaining a normal weight is a really complex and multifaceted challenge. So, we know that obesity is associated with many different factors. You can see here in the chart—psychological, genetic, physiological, metabolic, hormonal, sociocultural, environmental, behavioral. All of these aspects influence whether or not someone will become obese. And it's not-the obesity problem is not always solved by simply making a person eat less and exercise more. Certainly that can help, but there are many factors associated with overweight and obesity that we need to take into account when we're tackling this problem.
And so one particular thing I want to note here is that genes are involved; so your genetics, your predisposition for obesity, is involved in whether or not you will develop obesity or become obese or overweight. But, your genes do not solely determine your weight. A person can inherit a tendency towards being obese from their genes or their genetic makeup, but those genes are expressed (and by expressed I mean simply turned on or off) by interactions with lifestyle factors. So just because you have a genetic predisposition does not mean that you will automatically become obese or overweight. All of these factors, in combination with inactivity and constant access to high calorie foods, create a recipe for lots of obesity in this country. And so to be able to tackle the issue of obesity, you really have to be ready to tackle these complex and multifaceted issues.
Unfortunately we don't have complete control over everything that we saw on the previous slide relative to obesity. So we advocate a lifestyle approach to achieving and maintaining a healthy weight. What behaviors do you think are involved there? Of course if you guessed physical activity and energy intake you are correct! So, physical activity and energy intake, or your diet, are two behaviors that we focus in on when we're trying to manipulate lifestyle factors, or behavioral factors, for decreasing obesity.
And so, to start you might ask somebody to get baseline measures of how much they eat and how much they expend. So, very simply to get a sense for where they are on those, if you picture those scales that we saw a few slides back—are you in a negative energy balance, positive energy balance, or are you simply maintaining an equal energy intake and expenditure? In order to do this we might ask someone to complete food and physical activity logs for seven full days, and then look at what they did over those seven days. What did you eat? How many calories did you have per day? How many calories did you expend every day? And that can give a person a sense of whether they need to simply maintain what they've been doing or keep balancing the scale.
They also might need to unbalance the scale. So, maybe the person is in a positive energy balance where they're going to be gaining weight, even if they're not currently. If that's the case then we want them to unbalance the scale, right? We want them to either eat less or expend more through physical activity, or, ideally, do a combination of those two things.
And we'll note here that if you want to lose weight, one pound of fat is 3500 calories. So, ideally you use a combination of physical activity and caloric restriction to lose about a pound a week if your goal is to lose weight. And you do that by either reducing your caloric intake by about 500 calories per day or burning an extra 500 calories per day, or the third situation is, again the ideal, combining physical activity with caloric restriction. So you might increase your expenditure by 250 calories and decrease your intake by 250 calories, and then that gets you also in a balanced situation. So ideally we know that combining physical activity with caloric restriction works best, not only for losing the weight, but also maintaining your weight loss.
We know that physical activity is very important for fat loss, and although it doesn't create immediate losses necessarily (very fast quick losses like people often see with medications or a surgery), it is a good predictor-physical activity is a good predictor of maintaining your weight loss. Obviously physical activity burns calories, and we know that even moderate activity (such as walking) burns calories and can add up over the course of a day or a week or a month. And even very small weight losses, such as five to ten percent, can have lots of health benefits, including decreased blood pressure, cholesterol, decreases in your blood sugar levels, increased energy, mobility, self-confidence. So there are a wide range of benefits when people lose even just a small amount of weight—five to ten percent. And these are both physical and psychological.
We also know that physical activity also leads to waist loss, as you can see here on this slide. And that's really what we're talking about here—the loss of visceral fat.
Finally, we know that physical activity maintains your muscle mass, your lean muscle mass, and we know that increases in lean muscle mass is important for improving your metabolic rate and burning more calories, even when you're at rest.
So for all of these reasons, physical activity is a great way to help with fat loss.
Obviously healthy eating is also important for losing fat—weight or fat, for that matter. And here you want to think about both changing the types of food that you intake, or that you eat, and that's not just the type, but also the amount. So watch your serving sizes, choose those nutrient-dense foods that we talked about that give you the biggest nutritional bang for your buck that we heard about in chapter 7.
But you also want to think about your eating style modification. And by style we mean how quickly you eat, or the speed you eat. You want to eat slower and maybe try smaller meals or more frequent meals so that you avoid getting hungry. Certainly want to avoid eating under emotional situations where we tend to eat a lot more than we would in normal situations.
And finally, learn to enjoy the process of eating. So, focus on the process of making your food, enjoying the textures, the flavors. All of these things can help with eating for fat loss.
So far in this lesson we've talked only about your actual weight. But we also have a picture of our own bodies and what our own bodies look like called our body image, and this picture could be accurate or inaccurate. It could be positive or negative. And ultimately we want to have a healthy body image, and we get that by accepting our bodies the way they are, regardless of our weight, and also by focusing on healthy choices and not on how much we weigh or what the scale says.
Oftentimes a distorted body image can lead to unhealthy practices and, potentially, eating disorders. And although these disorders affect fewer people when compared to our problems with overweight and obesity, they're still important to understand. And so there are two that are listed here. There are certainly a whole host more, but we'll talk about two here.
The first is anorexia nervosa, and this is characterized by a distorted body image, self-starvation, and extreme weight loss. These people have an extreme fear of becoming fat, and actually think that they are fat even though oftentimes they are simply wasting away. And if left untreated it can not only result in weight loss but also in amenorrhea (or loss of a menstrual cycle for a woman), osteoporosis, muscle loss, and even potentially death if it's left untreated.
The second eating disorder here is bulimia nervosa, and this is controlled-characterized by uncontrollable cycles of binging-binge eating (or eating lots and lots of calories) followed by purging through either forced vomiting or the abuse of laxatives or diuretics. And so usually people with bulimia are in a normal weight range, unlike those with anorexia, but their weight might fluctuate due to that binging and purging cycle. And we know that that cycle puts a lot of strain on the body and has negative consequences.
We've covered lots of different topics in this chapter, so let's just take a moment to recap some take home points here. We began this lecture by talking about the trends in obesity from 1985 to 2010, and we saw that obesity has increased dramatically in the past 25 years, and we classify this as an obesity epidemic. We also talked about overweight and obesity and how both of these conditions are associated with many economic, social, and individual costs. We noted that this is a problem for children as well as adults. And we talked about how to tackle this complicated challenge, but we also talked about how physical activity and energy intake are two very important lifestyle factors that we do have some control over—a lot of control over—to help with the overweight and obesity problem. So although these aren't the only two factors that are associated with someone becoming overweight or obese, they certainly can play a big role in trying to reverse the epidemic.