In this lesson, we'll talk about the diabetes section of Chapter 14 as well as other information NOT included in your text about diabetes. We'll also define general terms used to describe diseases.
In this lesson we'll talk about the diabetes section of Chapter 14, as well as other information about diabetes that is not included in your text. We'll also define general terms used to describe diseases. After this lesson, you should be able to define disease-related terms such as epidemiology, prevalence and incidence. You should also be able to describe diabetes, distinguish between the different types of this disease and understand how diet, exercise and other lifestyle factors can play a role in preventing the development and complications of diabetes.
We'll spend the first few slides on this lesson going over general disease-related terms to make sure we're all on the same page when discussing common chronic diseases throughout the remainder of the semester, and so to begin, when we talk about how common a particular disease is, we often use terms like prevalence and incidence. Prevalence is simply the number of existing cases or the total number of people in a particular population who have a disease at a specific point in time. So for example, the number of people who currently have diabetes in the United States would be an example of a prevalence rate. Incidence is the number of new cases of a disease for a specific time period. So for example, you might see the number of new cases of diabetes this year. And so what you'll notice here is that prevalence is always going to be higher than the incidence of a disease because prevalence includes those new cases of the disease. Two other terms that we use very often are mortality, or the rate of death, or total number of deaths in a given time period, and morbidity, which is the state of disease or illness.
The field of study that examines the incidence and distribution of disease at the population level is called epidemiology, and incidence, like we just learned, refers to the number of new cases, and distribution refers to how these cases are spread out among the population. So for example, is the disease more common among people with specific characteristics? So do women get the disease more often than men? Does it occur more frequently with increased age? Are African Americans or Asian Americans more likely to get the disease? All of those are questions that the field of epidemiology might ask. Now variables that increase the probability of getting an illness or dying from that illness are considered risk factors, and some of these, such as smoking and physical inactivity, are behavioral choices, but some, such as race, obviously cannot be changed, and we call those non-modifiable risk factors. And we'll talk about the risk factors for diabetes later in this lesson, but what's important to note here about risk factors is that just because someone has a particular risk factor doesn't mean that they necessarily will develop the disease, only that they have an increased likelihood of developing that disease.
One of the primary goals of epidemiology is to be able to reduce the risk of disease through prevention, and there are three different types of prevention that we'll talk about. The first one is primary, and this is where we're trying to prevent a disease from ever developing, so we're trying to get people to choose not to smoke to help prevent them from developing lung cancer later in life. The second type is secondary prevention, and here the person already has the disease, but we're trying to prevent whatever disease we're talking about from worsening or from reoccurring again. So for example, we might have someone participate in a cardiac rehab program or change their diet to reduce the risk of a second cardiac event; that would be an example of secondary prevention. The third type of prevention is tertiary, and here we're just trying to reduce the negative impact of a disease that's already established. We're not trying to change the course of that disease, but rather just trying to reduce the negative impact that the disease has on the individual. And so, for example, we might have someone who has a chronic disease participate in physical activity just to improve the symptoms or to improve their quality of life, with the thought that physical activity is not going to cure the disease or that it's not going to keep the disease from progressing, but rather just improve the quality of the person's life. So these are the three different types of prevention that we'll talk about for both diabetes and the other diseases that we'll cover over the remainder of the semester.
So before we begin to define diabetes as a disease, let's just talk about some of the statistics. About 8% of the United States population has diabetes, and of those 8%, about 5% to 10% of those cases are type 1, and we'll talk about the differences between type 1 and type 2, but the majority of cases are type 2 diabetes; 90% to 95% of the cases of those 8% are type 2 diabetes. Diabetes affects people of all ages and all racial groups, although not necessarily in an equal manner, because there are higher rates for African Americans compared to Caucasian Americans, for example. We also know that with diabetes the risk of heart disease, death from heart disease, is 2 to 4 times higher for people with diabetes compared to adults without diabetes, so diabetes has complications not just in and of itself, but also for developing heart disease. And finally, we know that diabetes costs our nation a lot of money. The costs exceeded $174 billion in 2007, and as we'll see, those costs continue to increase, and that cost includes both direct costs of the disease as well as indirect costs such as lost productivity.
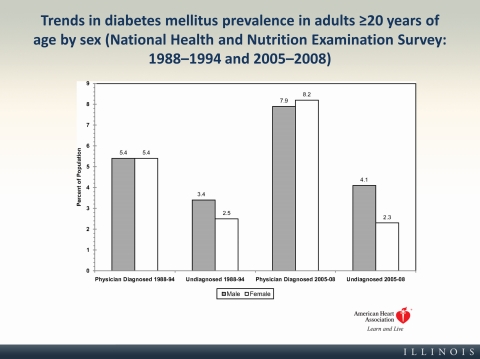
On this graph you can see the trends in the prevalence of adult diabetes in the US for both males and females, and you can see them for two different years, at the span of 1988 to 1994 on the two left-hand bars, and the two right-hand bars you can see 2005 to 2008. And what you see is that from the periods from 1988 to 1994, the diabetes rate was about 5% of the population, and now, in 2005 to 2008, it was about 8% of the population, and there's not a significant difference between males or females here that you see as well. So you see a pretty dramatic increase in diabetes. We'll talk about why this might be the case in a few slides.
Unfortunately, the rise in diabetes is also affecting the children in our country, and at quite an alarming rate. I'd ask you to watch this short video to learn more about the prevalence of diabetes in children.
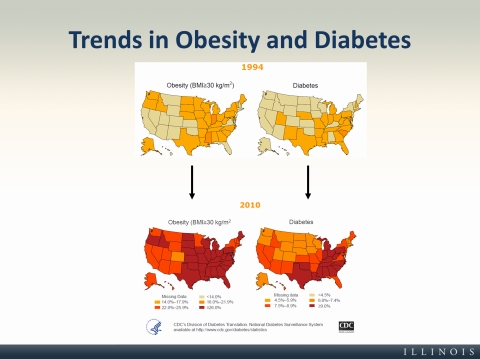
One of the major reasons we have seen an increase in the rates of diabetes in the United States is because of the increasing rates of obesity in our country. So here on these two graphs you can see pretty clearly that as obesity increased from 1994 to 2010, on the left side of these figures, diabetes also increased, and in a very similar fashion to the way obesity increased.
The hallmark of diabetes, regardless of whether we're talking about type 1 or type 2 diabetes, is high blood glucose levels, and as we'll learn in the next few slides, this can occur because of problems with insulin production, insulin resistance or both, and insulin is a hormone that's needed by our bodies, our body's tissues, to use the energy that we consume through food. So for example, insulin helps glucose get inside the muscle cell so the muscle can be allowed to do work, and this is particularly important when we're talking about being physically active, but also important for the health of all of the tissues in our body.
The first type of diabetes is called type 1, and we used to call this childhood-onset, although because type 2, as we'll see, is now occurring more frequently in children, we no longer use the labels of childhood and adult onset diabetes. And this type of diabetes is a chronic, lifelong disease where the pancreas produces little or no insulin to control blood sugar properly. It's an autoimmune disease where the insulin-producing beta cells in the pancreas are gradually destroyed and eventually fail to produce insulin. When they do this—the insulin is what, again, allows the glucose into your muscle cells and into the other tissues in your body—without that insulin, the glucose stays in your bloodstream, and so in order to treat type 1 diabetes, the person must have an insulin injection or a pump to survive, and we don't have any way to really prevent this from happening.
The second type of diabetes is called type 2, or non-insulin-dependent diabetes mellitus, and this type accounts, like we learned earlier, for the majority of all cases of diabetes, about 90% to 95% of all of our cases of diabetes. And in this type, the body doesn't have a problem producing insulin, but the body tissues, and specifically skeletal muscles, have developed a resistance to the insulin, so it's more difficult to move glucose out of the blood to be used as energy inside the muscle and other tissues. And lifestyle factors such as physical activity, diet, exercise, are the main ways to both prevent and to treat type 2 diabetes. So you should note here that both type 1 and type 2 diabetes both result in high levels of blood glucose, but this occurs for different reasons; there are different pathways that lead to this high glucose in the bloodstream.
We'll talk about the steps of type 2 diabetes development on the next slide, but first watch this video to see a visual and hear a description of how diabetes affects your blood sugar that was developed by the Mayo Clinic.
So as you saw in the video, type 2 diabetes there's no problem with the beta cells' production of insulin in the pancreas initially. Instead, the problem begins with insulin resistance in the muscles and in the skeletal muscles. The muscles are not taking in enough glucose because of this decreased sensitivity to insulin, so the glucose you saw gets let into the cell by that insulin molecule, and because the insulin's not able to do its job because the muscle is resistant, the muscle thinks it's being starved, doesn't have enough energy to do the work that it needs to do, and so these starved muscles send out a message to the liver to increase the glucose output, and this is the wrong message, because there's plenty; there's actually plenty of glucose, it's just that the muscle doesn't know that that glucose can't get into the cell. And so the liver then increases glucose output, which again is the wrong thing, but the muscle sent the wrong signal, and this results in excess sugar or glucose in the blood. To deal with that, the pancreas then increases production or secretion of insulin in attempt to reduce the blood glucose levels, and eventually these beta cells of the pancreas become overworked and dysfunctional over time from having to send more and more insulin out into the system to eventually allow some blood glucose to get into the muscle. When that happens, there's an impaired ability to secrete insulin that leads to elevated, continuously elevated, blood glucose levels, and you can have damage to healthy tissue. And so what you'll see here at the end is that as those beta cells start to become dysfunctional, type 2 diabetes starts to mirror type 1 diabetes and the effects of it, but it's important to note that that's not where it starts. Initially, in type 2 diabetes, there is no problem with the beta cells making enough insulin; it's just that the muscle is resistant to letting the insulin do its work. So these are the steps of the development of type 2 diabetes.
On this slide you can see some of the risk factors for developing type 2 diabetes mellitus, or some of the factors that are associated with an increased risk of developing the disease, and what you'll note is that some of these are lifestyle factors that can be changed, such as physical inactivity, smoking, but some of these are factors that you can't change; so for example, your family history. Specifically, if a parent or a sibling has had diabetes, you are more likely to get the disease as well. You also see in the list history of gestational diabetes. We'll talk about gestational diabetes on the next slide. It's simply a form of diabetes that occurs during pregnancy. And we also noted that African Americans are at higher risk compared to Caucasian Americans of developing diabetes. So all of these risk factors combined, some of which you can control and change, some of which you are essentially born with, are factors that we want to consider when thinking about whether or not someone will develop diabetes.
So like I said on the previous slide, gestational diabetes is a form of insulin resistance that develops during pregnancy, and it develops in about 18% of all pregnancies, and it's very important to make sure that women are tested for this disease so they can be treated, because if untreated, or it's poorly managed, what can happen is that the mother can develop high blood glucose levels, and then that blood glucose crosses the placenta, and the baby becomes exposed to these elevated blood glucose levels. And the baby's pancreas, by about 13 weeks, is able to make its own insulin, so insulin from the mother does not cross the placenta, but her blood glucose levels do, so the baby's pancreas responds to this extra glucose in the blood by producing increased insulin. Because of that extra glucose in the blood, the baby is getting more energy than it needs, and it stores that energy as fat just like we would, and that's why one of the conditions, if gestational diabetes is not treated, is called macrosomia, or a fat baby, and the baby has stored excess fat by being exposed to this excess glucose. All of this can be avoided if the mother is treated for this gestational diabetes, and usually it goes away in the mother after pregnancy, but the mother does have an increased risk of developing type 2 diabetes in the future. And some of the risk factors for developing gestational diabetes are someone's ethnicity—again, African Americans are more likely to develop this; if you have a history of diabetes already; and also if you're obese. And the treatment for gestational diabetes always includes some kind of special meal plan and regular physical activity, so some lifestyle changes, but it may also include daily blood glucose testing and also insulin injections, just depending on the person.
Listed on this slide you can see the symptoms of diabetes for both type 1 and type 2, and some of these include extreme hunger or thirst. When we talk about extreme thirst, this is really your body's way of trying to dilute the concentration of blood glucose. Fatigue or irritability—your body's cells are essentially starving because they can't get the glucose they need into the cell where it can do its work and be used as energy, and so you might feel fatigued or irritable. Infections—when you look on the type 2 diabetes side. High levels of blood glucose can impair our immune system and thus lead to more frequent infections. The tingling or numbness could be due to nerve damage that's caused by, again, having high levels of blood glucose. So you can see that really there are a wide range of symptoms, but all of which have to do with those high levels of blood glucose and having your body try to deal with those high levels of blood glucose.
Many of the costs associated with diabetes are because of the complications that can come with the disease if it's not treated or managed properly. And so we know that high levels of blood glucose are associated with an increased risk of heart attack or stroke, and in fact, people with diabetes are at least two times more likely to have a heart attack or a stroke compared to those who don't have diabetes. And about half of all people with diabetes have some form of neuropathy, which can affect many different areas of the body, and neuropathy—simply meaning nerve damage—can cause tingling, pain or numbness in your feet; it might cause problems with bladder control, your intestinal tract and digestion, or your genitals, such as erectile dysfunction. We also know that the kidneys, which filter our blood from waste products, become overworked, and diabetes is one of the leading causes of kidney failure in the United States, along with high blood pressure. You can also see eye complications with diabetes, such as glaucoma, which is problems due to excess pressure in the vessels leading to the eyes.
The good news about diabetes complications is that many of them are preventable if you follow some good steps towards preventing diabetes complications, and you can see some of those steps here. There are 10 steps that have been outlined by the Mayo Clinic as important. The number one of those is to practice good glucose control, or manage your glucose levels in your blood well. For every one percent that you can reduce you HbA1c, which we'll talk about in a minute—essentially it's just a marker of your blood glucose levels over the previous few months—you could reduce your risk of complications of diabetes by up to 35% depending on the complication. So 1% reduction in A1c, you get about a 35% reduction, up to 35% depending on the complication. We also know that many other health behaviors, such as quitting smoking, keeping your blood pressure and cholesterol low, taking care of your teeth, not drinking alcohol excessively. All of those things that are good for all of us are also very important in diabetes, and good preventative care, whether we're talking about regular exams, vaccinations, cleaning your teeth and gums, inspecting your feet for cuts or bruises; all of these are ways to prevent and reduce the impact of complications from diabetes. And so to see the full explanation for all of these preventative steps, read the full article that's listed here on the slide.
Because we know that physical activity is so important for both preventing diabetes before it occurs, or primary prevention, and preventing the progression or worsening of the disease, secondary prevention, we're going to talk about physical activity specifically here and the role it plays in diabetes. In the two studies focused on primary prevention, participants who had impaired glucose tolerance or people who were likely to develop diabetes but didn't have the disease yet reduced their risk of developing diabetes by 58% just by being physically active for about 150 minutes per week or meeting our national recommended guidelines, and losing a very modest amount of weight, about 5% to 10%. And so here we've learned that physical activity improves the body's response to insulin, and physical activity also helps people to maintain or reduce weight. So these are two ways that physical activity is associated with the primary prevention of diabetes, but in people who already have the disease—so we're talking about secondary prevention here—we also saw, through previous research, that an exercise training intervention showed that HbA1c—and again, those levels are simply a marker of your blood glucose levels over the previous couple months—those levels were lower in an exercise training group compared to a control group, and the exercise here was a little bit more intense than the 150 minutes we saw in the primary prevention studies. But together, these studies show the importance of being physically active, and in some cases also losing weight, to both prevent diabetes from ever occurring, or primary prevention, and also to improve cardiovascular health and to improve worsening of the disease or progression of the disease.
So the next question you might be asking is "Why does physical activity work to prevent type 2 diabetes?" and there are a few explanations here on this slide. The first is that being active increases the muscles' need for energy. This allows glucose to enter the cells through a pathway that is not dependent on insulin, so it's almost like an extra way to get glucose into the cell when you're being physically active. And as you can see on the slide, we also see increased insulin sensitivity after acute bouts of physical activity, so just after one bout of physical activity we see an increased need of the body to replenish muscle glycogen stores, and that effect can last for up to 48 hours. We also see increased insulin sensitivity that results from regular participation in physical activity, and this improves the functioning of the insulin pathway that allows glucose into the cell that we've talked about already in this lecture. And so all of these are ways that physical activity can help to prevent type 2 diabetes.
To end this lesson today, I want you to listen to the stories of Stephanie and Andy by clicking this link, and listen to how they talk about their new lives living with diabetes, and how they made lifestyle changes to manage their diabetes, and I think what you'll notice is that although it wasn't necessarily easy for them, it is possible to make lifestyle changes that can lead to better health, whether you have diabetes already or whether you're trying to prevent diabetes from occurring in the future.